
Actinic keratosis is a rough, scaly, or crusty growth on the skin that may develop into squamous cell carcinoma (SCC). Caused by sun damage, an actinic keratosis arises in the epidermis, or the top layer of skin, and usually in sun-exposed areas, such as the face, ears, bald scalps, forearms, and the backs of hands.
Actinic keratoses occur more frequently as a person ages. Individuals most at risk include those with a fair complexion and significant history of sun exposure. Incidence is higher in men than in women, as men tend to spend more time in the sun, use less sun protection, and have less natural protection from hair on the scalp. A diagnosis of actinic keratosis should be considered a warning sign that an entire area of skin has received too much exposure and damage from the sun, and that it is time to commit to sun safety and regular skin checks.
Classic actinic keratosis looks elevated and feels rough, like a wart or sandpaper.

BCC is the most common of all cancers. A majority of the estimated 3.5 million non-melanoma skin cancers in the United States in 2010 were basal cell carcinomas. BCC develops in the basal cells, the deepest layer of skin cells in the epidermis, and usually on skin that has been exposed to the sun. The face, ears, scalp, arms, and hands are most commonly affected. Generally, BCC is a slower growing skin cancer. Because BCC appears on areas like the face and neck that tend to be highly visible, it can greatly affect the appearance of facial features. Early detection and effective treatment with attention to cosmetic outcome are necessary to prevent the damage that may result from a BCC.
Individuals most at risk for BCC include those with a fair complexion, family history or personal history of skin cancer, and/or personal history of regular sun exposure.
Classic BCC is a growing or non-healing, flesh-colored papule (bump) that may resemble a mole.

SCC runs a close second to BCC in its rate of occurrence. Like BCC, it arises in the epidermis, or the top layer of skin, and usually on sun-exposed skin. Aggressive SCC also can spread beyond the skin into other parts of the body, and it is more likely to do this than BCC. Early diagnosis and proper treatment are an important priority.
Individuals most at risk for SCC include those who have had sun exposure throughout their lives, organ transplant patients, and/or those with immune deficiencies.
Classic SCC is a scaling, growing, irregular, thickened plaque that occasionally may bleed.
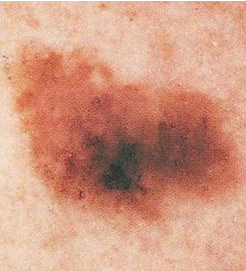
Melanoma is the most serious of the common skin cancers. It arises in the melanocytes, the skin cells that give your skin its color. Though melanoma arises in the skin, its natural progression is to metastasize (spread) to the lymph nodes or other parts of the body. When melanoma is detected and diagnosed early, with the initial skin lesion still relatively thin, surgical treatment may result in a complete cure.
When melanoma has had time to thicken and spread, however, curing the disease becomes much more difficult, as melanoma generally has proven resistant to traditional cancer treatments, such as chemotherapy. There is hope for a cure, and recent studies with a biologic agent known as Yervoy (ipilimumab), approved by FDA in March, 2011, has shown encouraging results in patients with inoperable / metastatic melanoma. This biologic agent employs gene therapy to enable the body’s immune system to combat the disease.
Anyone can develop melanoma, at any age. However, the following factors increase risk:
- Family history of melanoma
- History of persistent sun exposure and sunburn
- Light-colored skin, hair, and eyes
- Tanning beds – increase incidence of melanoma dramatically, especially in young adults
Symptoms – Remember: ABCDE
- A is for Asymmetry (Is one half of the spot different from the other half?)
- B is for Border irregularity (Is it oddly shaped or different from a regular round/oval mole?)
- C is for Color (Do colors vary across the spot, including tan, brown, black, red, white, and blue?)
- D is for Diameter (Is it larger than the diameter of a pencil eraser – 6 mm?)
- E is for Evolving (Is it new, or has it changed?)
Less Common Skin Cancers
Merkel Cell Carcinoma is a rare and aggressive form of skin cancer. It arises from Merkel cells in the lower part of the epidermis. Merkel cells are similar to nerve cells and give the skin “touch” sensation. Treatment involves a team approach from physicians with significant experience with the disease.
Atypical Fibroxanthoma is thought to arise from the dermis, which is deeper than the epidermis, the source of most other skin cancers. It classically appears on the face or scalp as a reddish, sometimes glistening plaque (broad, raised area on the skin).
Microcystic Adnexal Carcinoma is thought to be derived from cells that produce the adnexal structures, such as hair follicles and sweat glands in the skin. It classically occurs on the face. It may have a deceivingly benign appearance and may be mistaken for a common melanocytic nevus (mole).
For more information about your diagnosis
Detailed information can be found at www.dermsurgerystl.fromyourdoctor.com.